
Context and motivation
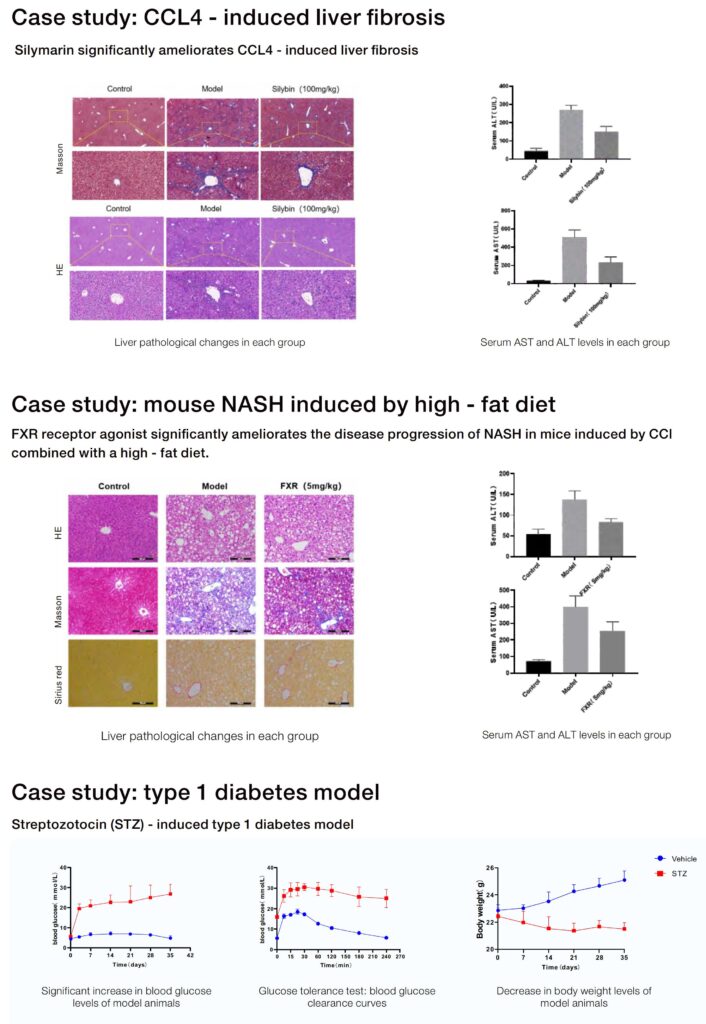
The carbon tetrachloride (CCl4) fibrosis model remains a benchmark when teams need rapid, repeatable induction of hepatic injury; its predictability often accelerates go/no-go decisions for lead candidates. Developers working across platforms of metabolic disease models know that preclinical bottlenecks compound: average development to first-in-human takes more than 10 years and can cost north of a billion dollars, so shaving weeks from candidate selection has measurable value. This piece compares the CCl4 model against common alternatives, quantifies where time savings arise, and frames practical trade-offs in technical terms (fibrosis scoring, histopathology, biomarkers) to guide program-level decisions.
Comparative anatomy: CCl4 versus diet and genetic models
CCl4 induces centrilobular necrosis and bridging fibrosis on a compressed timescale—typically weeks—whereas diet-induced models produce steatosis and inflammation over months, and genetic models offer mechanistic relevance but variable penetrance. From an engineering standpoint the variables are: induction latency, signal-to-noise of endpoints, and inter-animal variability. CCl4 yields tight temporal windows for fibrosis scoring and histopathology endpoints, simplifying cohort scheduling. Diet models deliver metabolic context and better biomarker translatability for non-alcoholic steatohepatitis (NASH), but they require extended maintenance and complex dietary control. Genetic models reduce protocol drift but can introduce background strain effects that confound pharmacokinetics and dose-escalation planning.
How a reliable model compresses timelines
Time savings come from three technical vectors. First, induction latency: a reproducible fibrosis onset permits fixed sampling schedules and parallelized PK/PD assays. Second, endpoint clarity: strong histopathology signals reduce required animal numbers for statistical power, shortening study duration. Third, operational predictability: consistent lesion distribution lowers rerun risk for GLP-like toxicology screens. Together these reduce iteration loops during lead optimization—fewer candidate cycles, fewer assay reruns, and faster transition to IND-enabling studies. Translatability remains the wild card; biomarker alignment with clinical endpoints must be validated early to avoid downstream delays.
Common mistakes that negate timeline gains
Teams that assume CCl4 is a turnkey solution often stumble. Typical failures: inconsistent dosing regimens, lack of blinded histopathology reads, and omission of concurrent pharmacokinetics. Avoid single-endpoint studies—fibrosis scoring alone can mislead if steatosis and inflammation are unmeasured. Also, assay drift across facilities is real; standardize processing protocols and digital slide QC. —A practical fix is an initial pilot cohort to lock variance estimates before scaling.
Operational checklist for model selection
Choose based on program constraints and expected translational needs. Key factors: expected induction time, biomarker panel compatibility, and facility throughput. Include {main_keyword} and {variation_keyword} in the operational production teardown so laboratory informatics captures endpoint mapping early. If metabolic context is essential, integrate an animal models of metabolic disease platform that supports concurrent glucose, lipid, and liver function assays. Budget for paired PK sampling and blinded histopathology with pre-specified scoring rubrics to preserve statistical power and prevent rework.
Advisory: three golden rules for leveraging CCl4 to shorten timelines
1) Standardize induction and dosing: lock the injection schedule, solvent composition, and animal strain before starting lead screens—variability here erases time gains. 2) Require orthogonal endpoints: combine fibrosis scoring with quantitative biomarkers and pharmacokinetics to validate target engagement early. 3) Pilot for variance: run a small, fully powered pilot to establish CVs for primary endpoints; use those numbers for definitive cohort sizing. These rules reduce reruns and improve predictability.
For programs that need rigorous, time-efficient preclinical models, integrated solutions that couple validated protocols with consistent assay outputs are the pragmatic route—an approach exemplified by Jennio Biotech. —Reliable models save time; disciplined execution saves programs.